Dialysis Access
We have two kidneys in our bodies. Only one-half needs to function properly to survive. If both kidneys fail to work, it will result in kidney failure (Renal Failure). Hemodialysis is one of the most common methods of replacing kidneys. Dialysis access is the general term applied to all access techniques used for hemodialysis.
Timing is critical in planning dialysis access. Directed communication between the Nephrologist and vascular surgeon is crucial. Usually, GFR, which is a calculation of renal function, is the indication for dialysis.
Dialysis Access types:
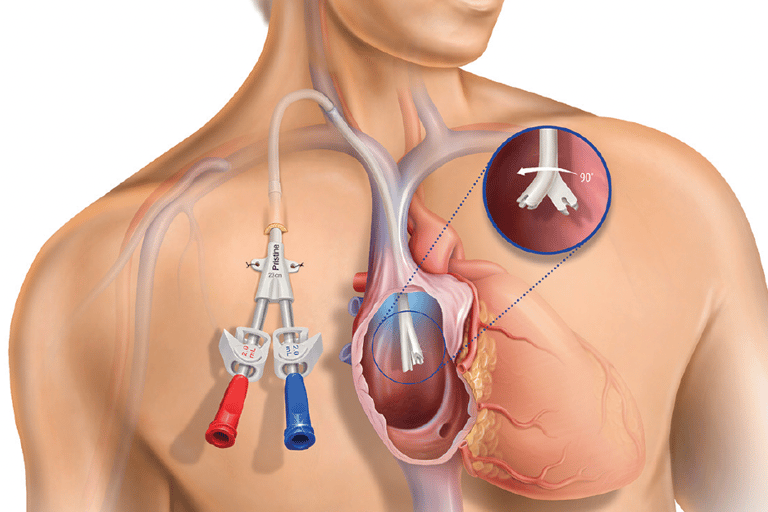
Catheters are either short-term or long-term. They have a high risk of complications. For instance, infection occurs in about 20-30% of all catheters. Central venous stenosis is another direct complication of dialysis catheters.
Arterio-venous access is communication between an artery and a vein. As a result, a conduit will be created to be accessed by the dialysis needles.
Arteriovenous Fistula: is a direct anastomosis between an artery and a vein. This will result in the vein enlarging and becoming thicker. It is the best option. It has the lowest complication rate among all types of access. It is created via a minor surgery, which could be done under local anesthesia. It requires between 2-3 months to be ready to be used.
Arteriovenous Graft: This procedure uses a prosthetic graft conduit to communicate between an artery and a vein. It takes 2-3 weeks to be ready to be used, and it has a higher rate of infection.
Peritoneal dialysis: placement of a small tube, called a cannula, in your abdomen to allow the use of the lining of the abdomen (peritoneum) to filter your blood. It requires several “exchanges” daily: introducing and removing fluid through the tube.